


Fillable PVC (Partial Volume Correction) Phantoms
Phantech’s Partial Volume Correction (PVC) phantoms are used to generate recovery coefficient (RC) calibration curves. By comparing the measured activity concentration in each sphere to the known activity concentration, one can characterize the signal recovered as a function of sphere size (simulating tumors & organs) by an imaging system and then apply a correction factor. Quantitative accuracy is critical for molecular imaging research and theranostic personalized medicine.
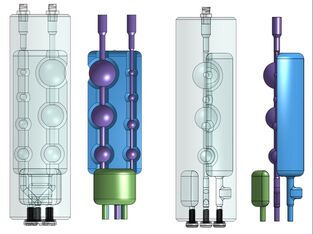
Designed with one continuous channel connecting numerous precise spherical or ellipsoidal volumes, Phantech’s PVC phantoms allow for quick, easy and safe filling.
- Available Sizes
- Automated Analysis
- Common Applications
- Customization
- What are Partial Volume Effects (PVEs)?
- Why do I need to correct for PVEs?
Phantech PVC phantoms are available in 3 standard sizes: 27, 34 and 49mm outside diameter. Customization is possible!
Outer Diameter (mm) Sphere Diameters (mm) Volumes (mL)* Product No.
27 2.5, 3, 4, 5, 7.5, 10, 12 2.43, 1.79, 10.36 PVC27-GrIT
34 3.8, 5, 6.2, 7.8, 9.8, 12.4, 14.2, 15.6 6.10, 3.41, 19.36 PVC34-GrIT
49 3.8, 5, 6.2, 7.8, 9.8, 12.4, 15.6, 19.6, 24.8 16.64, 11.08, 59.00 PVC49-GrIT
*Volumes match the figure below, including sphere void chain (purple), reference volume (green), and background (blue)
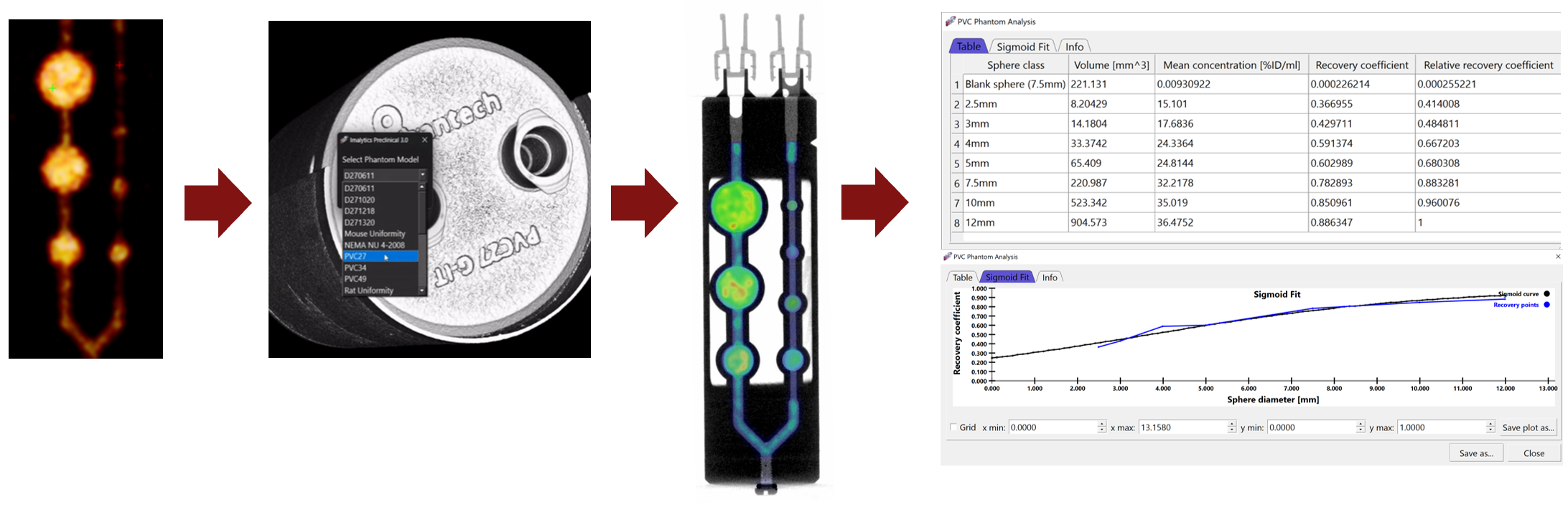
- Fill micro PVC phantom
2. Perform imaging scan
3. Load image file into Imalytics
4. Select the phantom from the dropdown menu
5. Generate and save report
- Recovery coefficient measurements
- Partial volume correction for dosimetry
- Co-registration (PET, SPECT, CT, optical, MRI, X-ray, MPI)
- Reconstruction optimization
- Multi-modality applications
- Standardization
- Image quality assessment
- Training
-
Marketing
Yes, we can customize our PVC phantoms. Customization options include a full 360 ̊ or half 180 ̊ sleeve for a “warm” spill-in compartment, a second channel of “micro-spheres”, and additional ellipsoidal PVC phantoms with varying aspect ratios (i.e. 1:2 & 2:3) to create a comprehensive 3D recovery coefficient correction curve.
Contact us at phanqual@radqual.com for custom requests!
PVEs are an inherent physical phenomenon present in all imaging systems largely due to sampling, blurring, motion, and physical hardware constraints. However, in nuclear medicine (particularly with PET and SPECT imaging), PVEs are compounded by a radioisotope’s finite positron emission energy and its respective inherent mean positron range. For a radioisotope with a relatively short positron range (ie. 18F in a static system, the intrinsic spatial resolution of the PET scanner will have a greater influence on partial volume effects (PVEs) than the positron range of the radioisotope. On the other hand, radioisotopes with relatively long positron ranges (ie. 124I, 89Zr) are largely responsible for PVEs due to the displacement of the originating positron emission voxel to the detected annihilation voxel. In either case, PVEs play a major role in the precision and accuracy of quantitative PET data, particularly with the degradation of measured radiotracer concentration in smaller structures using radioisotopes with long positron ranges.
PVEs contribute to imprecise and inaccurate quantitative data in ALL of the approximately 2 million clinical positron emission tomography (PET) and ~14.5 million single-photon emission computed tomography (SPECT) scans per year, and tens of millions of preclinical PET and SPECT scans per year. Clinically, not correcting for PVEs can have serious negative consequences on patient management and outcomes, including but not limited to, progressive disease, radiotoxicity of normal tissue in theranostic applications, erroneous staging and prognosis, and the inability to compare data in multi-site trials, which collectively contribute to increased healthcare costs. Preclinically, not correcting for PVEs can have serious negative consequences as well, including but not limited to, erroneous data interpretation and conclusions, radiotoxicity of normal tissue in theranostic applications, and the inability to compare data between institutions.